Oncology Research Projects
Oncology Research Projects

Completed projects
Liquid biopsies in lung cancer
Lung cancer is the deadliest form of cancer, and causes more lives lost than the other three most common cancers (breast, colon and prostate) combined. There have been major advances in lung cancer therapy in recent years, but mainly for patients with advanced, incurable disease. There has been less improvement for patients who undergo potentially curative therapy. Our research group is currently launching several projects aiming to improve treatment for these patients.
Current challenges
Surgery, radiotherapy, concurrent chemo- and radiotherapy are the main components of potentially curative lung cancer therapy. The treatment often causes severe toxicity, reduces physical function and ultimately affects patients' independence. For the health care services, such therapy requires a lot of resources. The major challenge is that a majority of patients who undergo potentially curative therapy experience relapse and die from their cancer within two years after treatment, and we are currently not able to identify those who are cured or those who relapse before treatment commences. Consequently, many patients undergo unnecessary, potentially toxic therapy.
Possible solutions
Liquid biopsies comprises one of the most promising approaches for developing an improved classification system. One reason is that it often is more difficult to obtain tumor samples in lung cancer than in other malignant disease. Based on our previous research and established methods, we aim to develop an integrative model based on a comprehensive assessment of tumor mutational landscape, ctDNA- and miRNA-analyses and complete clinical data that will predict the outcomes of each therapy patients receive, the risk of relapse and survival.
Hitherto, most liquid biopsy studies are relatively small, baseline cross-sectional studies. Our projects will have a longitudinal design which includes analyses of tumor, blood and urine samples collected before, during and after primary treatment and during follow-up - and complete clinical patient, disease, and treatment data.
Our research collaborative
These projects are interdisciplinary collaborations between researchers and clinicians from various disciplines involved in the exploration and diagnostics of lung cancer (pathology, molecular biology, oncology, lung medicine, radiology and bioinformatics). The research group cooperates closely with other Norwegian and Nordic research groups through the Norwegian Lung Cancer Group (NLCG).
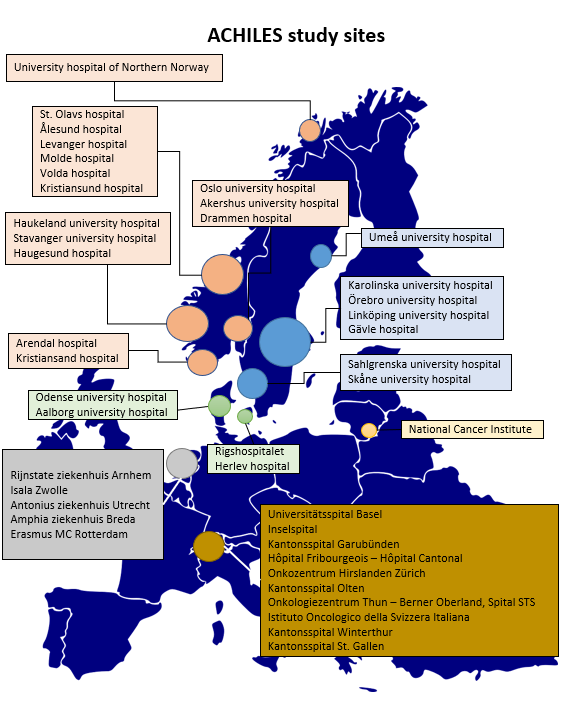
The ACHILES Trial
Achilleus in Greek mythodology was a hero of the Trojan war. He is the main character of Homer's Illiad. (forklar kobling mellom navn og trial)
The ACHILES Trial (Atezolizumab after concurrent chemo-radiotherapy versus chemo-radiotherapy alone in limited disease small-cell lung cancer) is a clinical trial with an estimated 160 randomized participants. Per 2020 105 patients has been included in the trial, in 41 hospitals and instutes all over Europe.
{kind=link}
Data collection manual updated
Version 5 of the data collection manual is now available. All sites will be notified of this update, please make sure to upload the new version in your ISF.
New protocol version
Version 1.3 of the protocol has been sent to all national coordinating investigators for approval. It has already been approved in Norway.
WebCRF changes
Patients randomized from 14th September, should be entered in a new crf, "ACHILES Main Study from Sept 14th 2020", regardless of TRT schedule. Patients who are already randomized should not be moved to the new CRF. The current CRF will be renamed "ACHILES Main Study until Sept 13th 2020", and you should continue to enter data in this CRF for patients included up until 13th September.
Data entry
Please remember to enter data in the WebCRF as soon as possible after study events, and no later than a week after each visit. If data is registered late, data-monitoring will be difficult to perform.
Below you will find answers to some of the most usual questions from site study personell. The answers are provided by the ACHILES study team and PI in Trondheim.
How are patients to be followed up after EOT visit if they have quit the study due to something else than progression?
- Patients who terminate use of atezolizumab for other reasons than progressed disease are to be followed up according to trial plan.
Invoicing
- Chapters five and eleven in your study agreement indicate procedures for invoicing, as well as rates for initiation, patient inclusion and randomization.
When should blood samples for biobanking be collected when recruiting patients who have started/completed radiotherapy?
- Wait until evaluation at week 12, as the purpose of these tests is to evaluate the effect of chemo- and radiotherapy. Remember to draw whole blood in addition to tests described at week 12.
How are patients to be listed in the WebCRF when they are included after chemotherapy / at randomization?
- All of the ACHILES induction part is to be completed. It is a requirement for inclusion after chemoradiotherapy to know what treatment the patient has received. Use labels for "Evaluation".
What does theme number in the Site Shipping Request Form mean?
- The theme number is an internal number at Roche which will not change for the ACHILES study. It stays the same for all shipment orders and all countries.
Which values are preferred when centrifuging urine?
- 4000g, 4C.
Delivery time and shelf life
- Shipment from the main depot in Germany to your pharmacy will take 3-4 days. Atezolizumab is durable for three years from April 2018.
Quantity of atezolizumab
- One injection vial per treatment. Each patient is to receive treatment every third week for one year.
How long can atezolizumab treatment be postponed?
- The protocol states that atezolizumab may be suspended for other reasons that toxiciy (e.g. surgical procedures) with sponsor approval. The investigator and the sponsor will determine the acceptable length of treatment interruptions. In practice the most important thing is not to administer atezolizumab with intervals less than three weeks. Whether some courses are postponed a few days or up to one week, is not critical.
If the patient is in poor condition, treatment can be postponed up to twelwe weeks, according to protocol.
Should patients who exit the study due to progression be followed up every 12 weeks as per the survival follow up?
- Patients who terminate use of atezolizumab due to progression (+ no clinical benefit / need for other therapy) are to be followed according to local routines (survival and relapse treatment).
Achiles trial office: achiles@stolav.no
Principal investigator: Professor Bjørn Henning Grønberg
TRIPLEX
More than 3300 are diagnosed with lung cancer every year in Norway, and 2200 die from the disease, accounting for more than 5% of all deaths in Norway. 13-16% of lung cancer patients are diagnosed with SCLC, small-cell lung cancer. Untreated, the prognosis is poor.
There are two main types of lung cancer, small-cell lung cancer (SCLC) and non-small-cell lung cancer (NSCLC). Approx. 13-16% of patients have SCLC. Untreated, the prognosis is poor (2-4 months), since SCLC grows more rapidly and metastasizes more frequently than NSCLC. Due to the aggressive biology, SCLC causes 4% of all cancer-related deaths.
Most lung cancer research focuses on NSCLC, and the poor survival rate for SCLC, the lack of research, progress and new therapies underscores the need for more research on this orphaned disease.
If you have questions and are a participant in the study, please contact your doctor or the study personell at your hospital. You can also contact the TRIPLEX Project Leader, Professor Bjørn Henning Grønberg.